
עבודה זרה כז, א
ישראל שמתו אחיו מחמת מילה ולא מלוהו
A Jew whose brothers died following their circumcisions, and was not circumcised....

In today's Daf Yomi, the Talmud considers whether a Jew who was not himself circumcised may serve as a mohel. This situation could arise when the newborn baby had older brothers who died from bleeding following their circumcisions. The young brother is then exempt from the mitzvah to be circumcised.
We first encountered this situation while studying Yevamot (64a) where cases of post-circumcision deaths are described. To understand the today's daf, we need to remind ourselves of the genetics of hemophilia.
X-linked Hemophilia A
יבמות סד, א
תניא מלה הראשון ומת שני ומת שלישי לא תמול דברי רבי רבן שמעון בן גמליאל אומר שלישי תמול רביעי לא תמול... א"ר יוחנן מעשה בארבע אחיות בצפורי שמלה ראשונה ומת שניה ומת שלישית ומת רביעית באת לפני רבן שמעון בן גמליאל אמר לה אל תמולי
It was taught: If she circumcised her first son and he died, and her second son and he too died, she should not circumcise her third son, so taught Rebbi. Rabbi Shimon ben Gamliel stated that she should indeed circumcise her third child, but [if he died] she must not circumcise her forth...Rabbi Yochanan said that there was once a case in Zippori in which four sisters had sons: The first sister circumcised her son and he died, the second sister circumcised her son and he died, the third sister circumcised her son and he died, and the forth sister came to Rabbi Shimon ben Gamliel and he told her "you must not circumcise your son" (Yevamot 64:)
The Talmud here is describing a disease that is affected through the maternal line (hence the four sisters - all of whom seem to pass this disease on to their male children). The disease is X-linked Hemophilia A; the term X-linked indicates that the faulty gene is carried on the X chromosome, which is men is always inherited from the mother. Hemophilia A is an X-linked recessive genetic disease, first described by the American physician John Conrad Otto, who in 1803 described a bleeding disorder that ran in families and mostly affected the men. John Hay from Massachusetts published an account of a "remarkable hemorrhagic disposition" in the New England Journal of Medicine in 1813.

Hay, John. Account of a Remarkable Haemorrhagic Disposition, Existing in Many Individuals of the Same Family. New England Journal of Medicine 1813:2;3;221-225.
If the mother is a carrier - as were each of the four sisters in Zippori - then she has a one in four chance of passing on the disease to a child, and that affected child will always be a son:
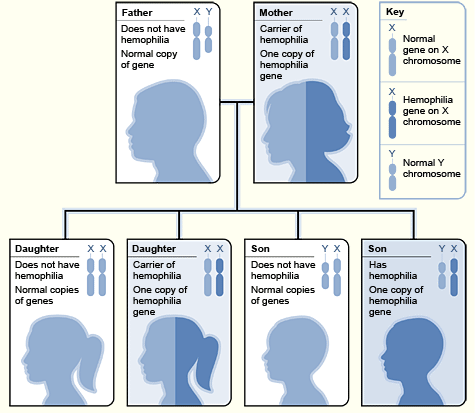
Courtesy NHLBI
In Yevamot, the rabbis argued over a technical point - that is, how many cases of bleeding are needed to establish a pattern. According to Rebbi (that is Rebbi Yehuda Ha-Nasi, c. 135-217 CE.) two cases were sufficient, while Rabbi Shimon ben Gamliel insisted on three cases before ruling that there was a life threatening pattern. Indeed the disease in boys must have been very perplexing, because (as you can see in the diagram above) not every boy would be affected. In fact, if the mother is a carrier and the father is not, there is only a 50% chance of a boy having hemophilia. It is this fact that perhaps explains the dispute between Rebbi and Rabbi Shimon ben Gamliel regarding how many children need to exhibit the disease before we can assume that any future male child will also have it. If every boy born in the family would have been a hemophiliac, Rabbi Shimon's ruling would have seemed unnecessarily cruel. But since by chance, half of the boys born might not have hemophilia, the need to demonstrate the prevalence of the disease (in a society in which its genetic foundations were not known) seems eminently sensible.
In Hemophilia A there are various genetic mutations that result in low levels of clotting factors. These levels may be only mildly decreased, or so low that severe life threatening hemophilia results. It is treated with transfusions of clotting factors which restore the levels to normal. Although these transfusions must be given several times a week in those with severe disease, there is hope that recombinant clotting factors can lengthen the time between the needed transfusions.
Later in Yevamot, the Mishnah records the case of a priest who was not circumcised - because of the deaths of his brothers when they underwent the procedure. So this law was certainly practiced, and the Talmud records not only the earliest known description of hemophilia, but the emphasis on the preservation of life as a normative Jewish practice.
רמב׳ם משנה תורה הל׳ מילה ב, א
הַכּל כְּשֵׁרִין לָמוּל. וַאֲפִלּוּ עָרֵל וְעֶבֶד וְאִשָּׁה וְקָטָן מָלִין בְּמָקוֹם שֶׁאֵין שָׁם אִישׁ
Everyone is qualified to perform the operation of circumcision. Where there is no adult circumcised male, (Israelite), it is performed by an uncircumcised Israelite, a bondman, a woman or a minor.
[Repost from Yevamot 64a.]


